Travell and Simons (J. G. Travell & Simons, 1983, 1992) and Cyriax (Cyriax, 1977) advocate the use of trigger point injection as an effective method of treatment, but this treatment is neither appropriate nor legal for rehabilitation clinicians. When an active trigger point does not respond to the treatment techniques presented here, it may be useful to refer the patient to a physician who can inject the site.
Trigger point treatments using Travell and Simons’ techniques are direct methods. Three primary methods of myofascial trigger point treatments are discussed briefly here. For additional information, refer to the Travell and Simons texts (J. G. Travell & Simons, 1983, 1992), the source of the techniques described next.
Fluorimethane as a vapocoolant spray was formerly used as a common treatment for myofascial trigger points. Now that we are more aware of the harm that chlorofluorocarbons cause to the atmosphere, fluorimethane is no longer used. A cold spray without fluorimethane is commercially produced and available. Some clinicians who are environmentally concerned have replaced cold spray with ice stroking using an icicle. An “icicle” is made by placing a tongue depressor in a cup of water and freezing the water. Before applying the icicle to the skin, the paper or styrofoam cup is torn back and covered with thin plastic wrap to avoid getting any cold water drips on the patient’s skin; keeping the skin dry throughout the treatment maintains the contrast between the warm skin and the cold ice. Travell and Simons (J. G. Travell & Simons, 1983) indicated that this technique of applying ice or vapocoolant followed by a stretch was the most effective technique to treat trigger point pain.
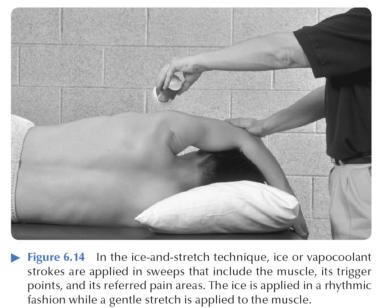
Before application, the patient should be instructed to relax. Applying just enough pressure on the trigger point area to produce the referred pain may help the patient understand why your treatment is not being applied directly to the area of pain. The patient is placed in a comfortable position with the skin exposed and the body part supported to permit full relaxation. Before treatment, the part is moved through its range of motion so you and the patient can judge changes made by the treatment. With the muscle anchored at one end, the ice or vapocoolant spray is applied in a sweeping motion in parallel strokes in only one direction over the length of the muscle and then over the referred pain pattern. As the ice or vapocoolant is applied in a rhythmic, unhurried fashion, a slow, continual, passive stretch is applied progressively to the muscle. Any one area of the skin should receive only two to three strokes of cold before rewarming to achieve optimal results of the ice-and-stretch technique (figure 6.14). The rate at which the ice or vapocoolant is moved over the skin is approximately 4 in/s (10 cm/s). The stretch force should be light enough that it does not elicit a stretch reflex from the muscle but strong enough to be effective. As a muscle releases, you must be able to detect the relaxation and place the muscle in a new stretch position that takes up the slack and provides the same level of tension on the muscle. The application and release of the stretch force should be done smoothly and gradually, not quickly. A hot pack can be immediately applied to further relax the muscle. The patient can also assist the stretch by contracting the antagonist, but you must monitor the contraction so as to prevent a co-contraction of the agonist and antagonist. The cold-and-stretch technique can be repeated for several cycles after the skin has been rewarmed, depending on the results of treatment, the patient’s response, and desired goals.
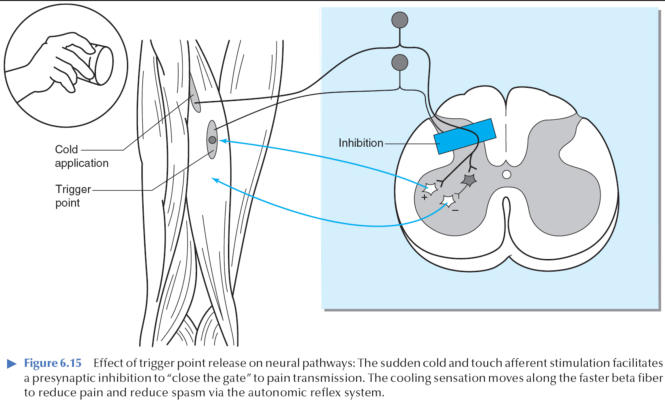
It is believed that this technique is effective because of two mechanisms, although they have not been confirmed through research. The gate theory of pain presented by Melzak (Melzack, 1973) and the modified gate control theory advanced by Castel (Castel, 1979) postulate that sudden cold and touch sensations inhibit the pain cycle by blocking transmission of pain signals. Active trigger points activate the pain-spasm response. Ice stroking inhibits the pain-spasm cycle and allows the muscle to respond to the stretch (figure 6.15).
The second factor is mechanical: If a muscle is stretched, its sarcomere elongates and releases the actin and myosin elements enough to end the sustained muscle fiber contraction.
Another myofascial trigger point release is ischemic compression. In this technique, pressure is applied slowly and progressively over the trigger point as the tension in the trigger point and its taut band subsides (J.G. Travell & Simons, 1983). Pressure is maintained until the tenderness is gone or the tension is released. This is followed by stretching the muscle. Before application, the patient should be informed that some discomfort may occur. Hanten et al. (Hanten, Olsen, Butts, & Nowicki, 2000) found that this technique of ischemic compression followed by stretching provided the best and most effective decrease in trigger-point pain levels.
A third technique is stripping massage, a deep-stroking massage applied with minimal lubrication on the fingertips. A firm pressure is used along the length of the taut band (J.G. Travell & Simons, 1983). The pressure increases progressively with each successive pass along the muscle. A milking movement from the distal to proximal end of the muscle goes over the trigger point at the rate of about 1 in. (2.5 cm) every 3 s. As the effects of the technique become apparent, the taut band relaxes, the trigger point nodule softens, and the area ceases to be tender and no longer refers pain.
The ischemia produced by the pressure of the ischemic compression or stripping massage techniques is believed to cause a reflexive hyperemia that returns the site to a normal condition (J.G. Travell & Simons, 1983).
The PNF techniques of contract-relax and reciprocal inhibition, which were introduced in chapter 5 and are discussed further in chapter 7, are also effective when combined with soft tissue mobilization in relaxing myofascial trigger points (Godges, Mattson-Bell, Thorpe, & Shah, 2003). In addition, various other techniques are used in the treatment of myofascial trigger points. Modalities such as hot packs, ultrasound, and electrical stimulation are also frequently used as adjuncts to enhance the effectiveness of treatments.