|
Rehabilitation of impingement
This is an excerpt from Assessment and Treatment of Muscle Imbalance: The Janda Approach by Phil Page, MS, PT, AT, CSCS, Clare C. Frank, DPT, and Robert Lardner, PT.
|

Rehabilitation rather than surgery is recommended for secondary impingement (Brox and Brevik 1996; Kronberg, Németh, and Broström 1990; Michener, Walsworth, and Burnet 2004; Morrison, Frogameni, and Woodworth 1997). Patients with primary impingement (type II and III acromion), however, have only a 64% to 68% success rate with conservative treatment (Morrison, Frogameni, and Woodworth 1997). While rehabilitation and arthroscopic surgery improve impingement symptoms equally (Haarh et al. 2005; Haarh and Andersen 2006), rehabilitation is less costly (Brox et al. 1993).
In a systematic review, Michener, Walsworth, and Burnet and colleagues (2004) found strong support in the literature for therapeutic exercise of the rotator cuff and scapular muscles as well as for stretching of the anterior and posterior shoulder. Furthermore, exercise is more effective when combined with joint mobilization (Michener, Walsworth, and Burnet 2004; Senbursa, Baltaci, and Atay 2007). The following are impingement rehabilitation recommendations with evidence-based rationale:
- Integrate the entire upper-extremity chain during exercise. This facilitates the kinetic chain from the hand to the spine (Burkhart, Morgan, and Kibler 2003; Kibler 1998b, 2006; McMullen and Uhl 2000). Figure 13.5 illustrates exercises that integrate the whole kinetic chain.
- Include hip and trunk stabilization exercises. This facilitates force transmission and proximal stabilization between the upper extremity and the trunk (Burkhart, Morgan, and Kibler 2003; Kibler 1998b, 2006; McMullen and Uhl 2000).
- Isolate the rotator cuff and scapular stabilizers first, before performing multijoint movements. Performing multijoint shoulder movements does not increase the strength of smaller single-joint muscles such as the rotator cuff (Giannakopoulos et al. 2004). Strengthening exercises isolating the rotator cuff should be performed first (Jobe and Pink 1993; Malliou et al. 2004).
- Exercise in the scapular plane. The scapular plane offers the most balanced position of the capsule and provides ideal joint centration during elevation (Borsa, Timmons, and Sauers 2003).
- Exercise both shoulders. Abnormal muscle activation often occurs in both the involved and the uninvolved shoulder (Cools et al. 2003; Cools, Declercq et al. 2007; Wadsworth and Bullock-Saxton 1997).
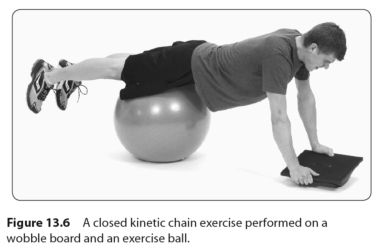
- Include neuromuscular exercises such as closed kinetic chain exercises and PNF. Patients with impingement demonstrate reduced proprioception (Machner et al. 2003) and so require proprioceptive rehabilitation (Ginn and Cohen 2005; Kamkar, Irrgang, and Whitney 1993; Smith and Burnolli 1989). Figure 13.6 illustrates a closed kinetic chain shoulder exercise for improving proprioception (Naughton, Adams, and Maher 2005).
- Stretch the posterior shoulder when internal rotation is limited. The posterior capsule is often tight in athletes with impingement, limiting internal rotation and follow-through (Myers et al. 2006; Tyler et al. 2000). The cross-body stretch (see figure 13.7) improves internal rotation in subjects with posterior shoulder tightness (McClure et al. 2007).
|
|